Today
See what needs attention across the clinic.
For clinic owners and operators
Follicle Intelligence gives clinic owners one operating view across enquiries, patients, consultations, surgery, imaging, workforce and outcomes — without requiring every existing system to be replaced on day one.
Follicle Intelligence connects commercial activity, patient care, surgery, staff, imaging and outcomes so clinic owners can see what is happening, where performance is being lost and what needs attention.
Built around the realities of operating modern hair restoration clinics.
Owner visibility
Today priorities, front-desk flow and calendar coordination — the operating views that keep a clinic moving.
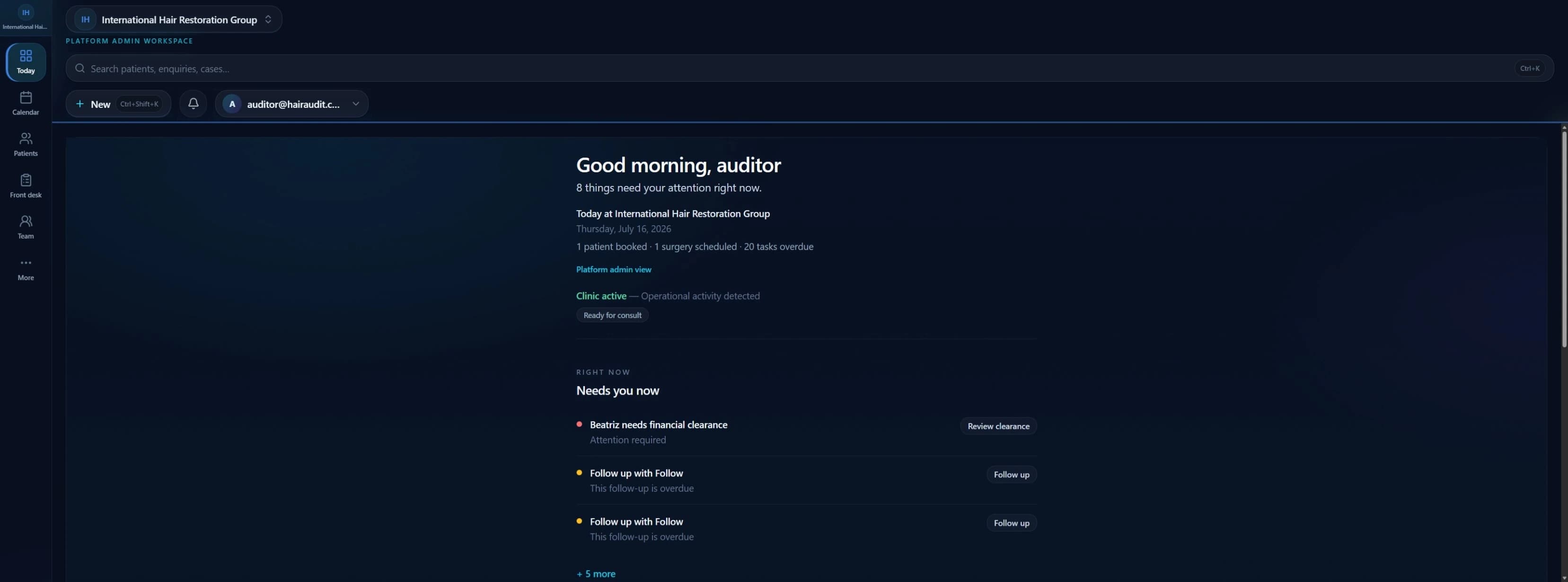
Today
See what needs attention across the clinic.
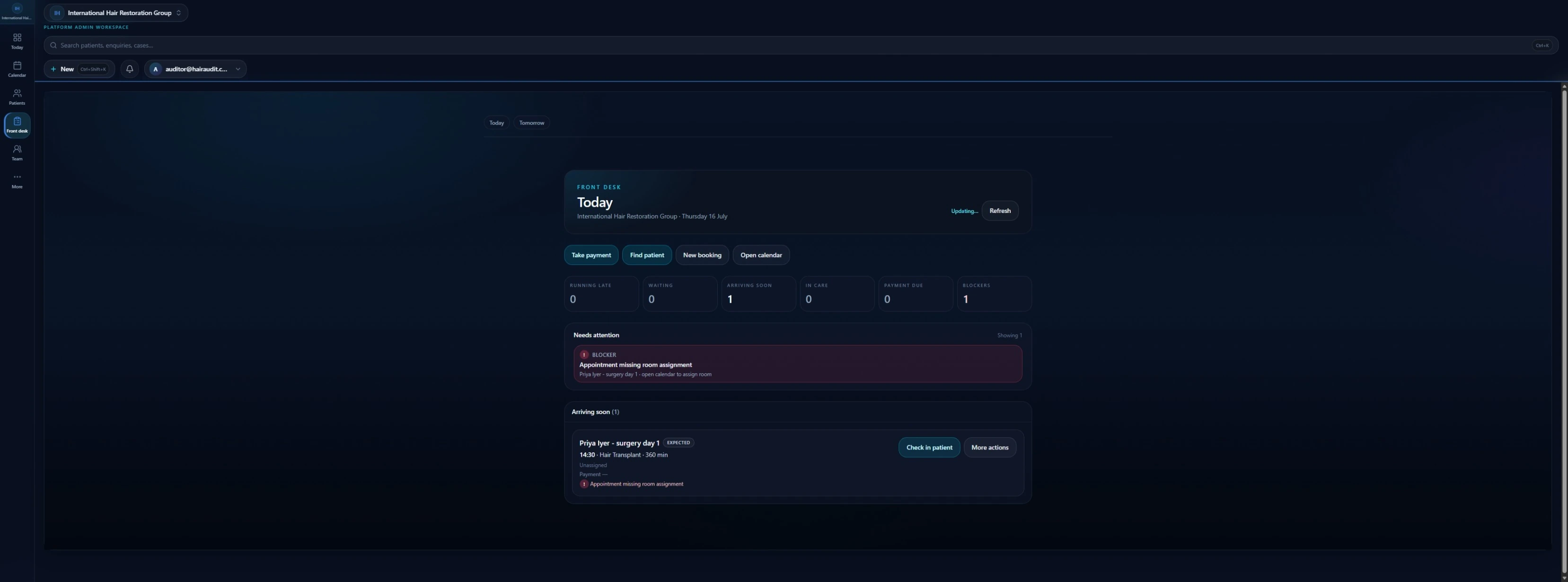
Front Desk
Manage arrivals, delays, blockers and patient flow.
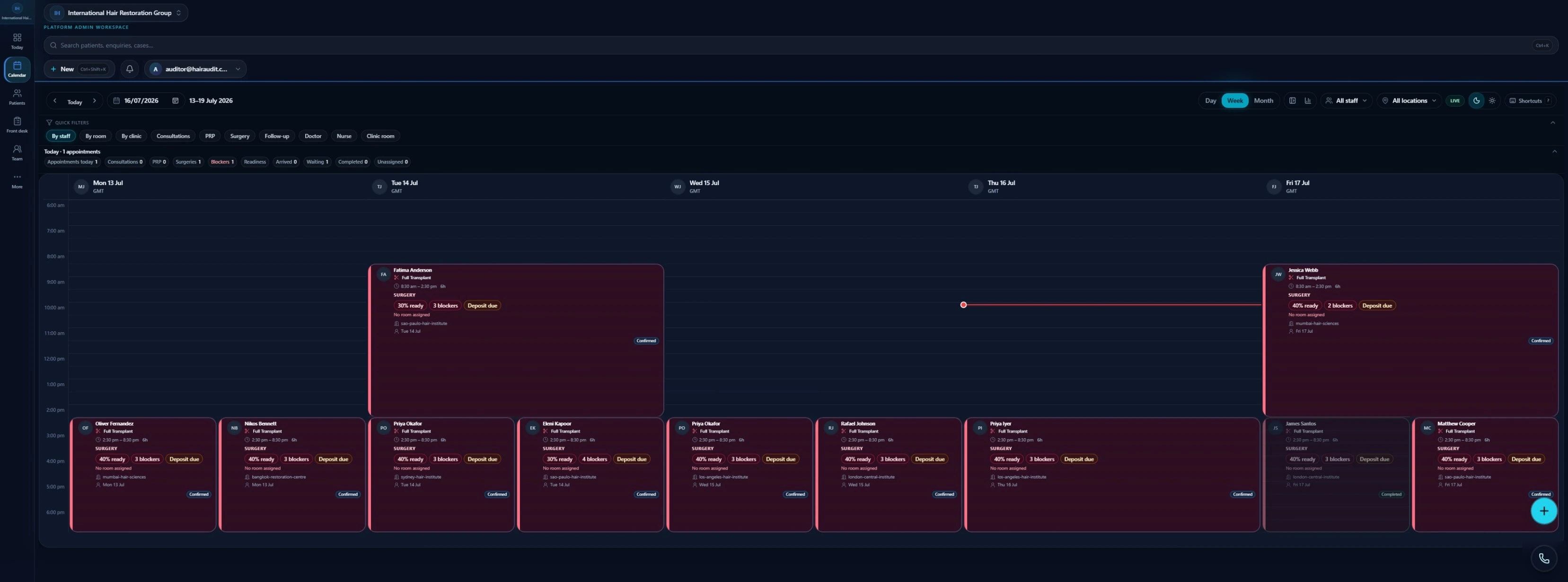
CalendarOS
Coordinate consultations, treatments, teams and surgery.
Interface shown with demonstration data.
The operational problem
They have a collection of systems, spreadsheets and staff processes that do not share the same patient journey. That fragmentation affects commercial performance, patient experience, staff accountability, clinical continuity, management visibility, multi-site consistency and long-term outcome measurement.
Website forms, HubSpot, email, phone, social, referrals, spreadsheets and personal inboxes make ownership unclear — so follow-up becomes inconsistent and conversion hard to trust.
Commercial context sits in one place while consultation notes, imaging, surgery planning, follow-up and outcomes sit elsewhere — creating duplicate data and weak handovers.
Headline revenue is not enough. Owners need to see where patients leave the journey, whether follow-up is completed, whether surgery is ready, and whether sources create long-term value.
Tasks in personal inboxes, informal follow-ups, spreadsheet rosters and conversation-based readiness create operational risk and break when staff leave.
Fear of lost history, duplicate records, training burden and downtime often freezes progress — even when fragmentation is obvious.
What changes with FI
Follicle Intelligence is a hair restoration operating system. The point is clearer ownership, one connected patient journey and better day-to-day coordination — not more disconnected software.
Clear assignment, visible stage, follow-up responsibility, contact history, and lost or converted review — so demand does not depend on individual memory.
Enquiry, consultation, imaging, treatment, surgery, follow-up and outcome share the same identity rather than being recreated in separate tools.
Calendar, front desk, patient readiness, procedure preparation, team visibility and operational attention points stay closer together.
Role-based access, roster visibility, readiness, competency, training and assigned responsibility reduce reliance on informal heroics.
Planning, graft and hair data, team involvement, imaging, follow-up and outcome audit can stay on the same patient thread.
Enquiries, conversion, follow-up, patient movement, surgery readiness, staff capacity, operational risk and outcomes become easier to review — with financial and reporting depth expanding over time.
Connected operating systems
These are not six disconnected products. They are everyday clinic systems that share the same operational spine. Module depth varies by deployment status — see Platform Progress for current maturity.
LeadFlow
Enquiry capture, pipeline, ownership and follow-up connected into the patient journey — with progressive HubSpot connect, coexistence or staged transition when needed.
ClinicOS
Scheduling, services, appointment lifecycle and day-to-day clinic rhythm for multi-site operators.
WorkforceOS
Roster, readiness, competency and workforce planning so capacity matches assigned work.
PatientOS
Longitudinal patient record and journey continuity across commercial and clinical activity.
ConsultationOS
Structured consultation assessment, planning and handoff into treatment or surgery.
ImagingOS
Standardised capture, comparison and longitudinal visual records.
SurgeryOS
Procedure planning, day-of coordination, graft and team activity on the same patient thread.
AuditOS
Outcome measurement, procedure audit posture and review-ready evidence pathways.
AnalyticsOS
Commercial, operational and outcome intelligence built from structured events — expanding as capture depth grows.
Connected patient journey
01
Capture, ownership and follow-up
02
Assessment, plan and expectations
03
Preparation, procedure and team activity
04
Care continuity and next actions
05
Imaging, review and learning
Progressive adoption
Clinics can start with the workflows that matter most, keep selected systems connected, and expand as confidence grows.
Connect, transition or replace — at a pace that protects clinic continuity.
01 · Mode
Keep selected systems connected to FI.
02 · Mode
Use FI alongside existing systems during a controlled adoption period.
03 · Mode
Move selected workflows and data into FI in verified stages.
04 · Mode
Use FI as the primary operating environment within the agreed scope.
Clinics using HubSpot can begin by connecting selected workflows, transition active contacts and leads in stages, or progressively move CRM activity into LeadFlow. The same progressive principle applies to booking, calendar and operational tools where supported.
See how controlled transition worksMigration continuity
FI is designed to support a controlled transition rather than an abrupt cutover. Existing systems can remain in place while selected workflows and records are verified and moved in stages.
What the owner can see
Visibility grows with structured capture. Not every signal is fully operational for every clinic today — maturity is labelled honestly.
Active in defined clinic workflows within approved deployment scope.
Foundations exist; depth and consistency continue to grow.
Strategic capability direction — not claimed as fully operational product today.
Multi-site groups
Designed to support multi-site groups that need shared operating standards without erasing local ownership.
Why value compounds
As FI connects acquisition, consultation, treatment, surgery, imaging, workforce, follow-up and outcomes, the clinic gains a richer longitudinal history.
In most software, a converted lead becomes a closed record. In FI, that conversion becomes the beginning of the clinical and outcome journey.
Operational status
Follicle Intelligence is operating across defined clinic workflows, with several systems in controlled operational pilot and others progressing through advanced build and integration.
Deployed · Operational Pilot · Advanced Build · In Development · Research and Future Development
View Platform ProgressNext step
Improve enquiry follow-up, connect existing systems, standardise operations or plan a wider transition into the Follicle Intelligence operating system.